
- WHAT IS AN AORTIC ANUERYSM?
- WHAT ARE THE SIGNS & SYMPTOMS OF AN AORTIC ANEURYSM / DISSECTIONS
Chest pain- often radiating to the back or shoulder blades.
Back pain- frequently diagnosed as a spine problem.
Hoarseness of voice
Abdominal pain
Lower back pain
Feeling a pulse, soft mass in the abdomen
- AM I AT RISK?
- WHAT TO DO IF I HAVE AN ANEURYSM/DISSECTION?
- HOW ARE TAA/AAA TREATED?
- WHAT IS THE ANEURYSM CLINIC?
Aorta, which is the main artery in the body, transports blood from your heart to the rest of the body. Various important arteries arise from the aorta. As it courses through the chest, it is known as the thoracic aorta; through the abdomen, it is called the abdominal aorta.
Weakening of the aorta, due to atherosclerosis, trauma (injury) , genetic or hereditary defect in the tissue within the arterial wall can cause the aorta to bulge or expand; which is known as an aneurysm.
A thoracic aortic aneurysm (TAA) is a dilatation of the aorta in the chest, in the abdomen, it is known as an abdominal aortic aneurysm (AAA). Thoraco-abdominal aneurysms involve the major arteries in the abdomen (intestinal and renal); which are a major challenge to treat.
Another common aortic pathology is aortic dissection, where the aorta is split into two channels, causing intestinal, renal or limb compromise or in later stages aneurysmal dilatation.
Majority of aortic aneurysms are incidental detections on radiological investigations such as X-ray Chest/Spine, ultrasound, computed tomography (CT) and Magnetic resonance imaging (MRI).
When symptoms are present:
In cases of thoracic aneurysms/dissections:
In cases of abdominal aortic aneurysms:
If the aneurysm enlarges rapidly, it can burst and is known as a ruptured aortic aneurysm, which is life threatening. This requires immediate emergency care.
Ruptured aneurysms should be avoided, since the results of treating them are very poor.
Hence early detection and treatment of aneurysms are mandatory.
Risk factors for developing an aneurysm are family history, smoking, heart disease, high blood pressure and high fat diet.
They are known to occur more frequently in the older population, although thoracic aneurysms and dissections are known to occur in younger individuals also.
The most significant risk factors are smoking, history of heart disease and a family history. If you are in the high risk category, screening tests such as ultrasound and computed tomography can be done.
If there is a high risk of an aneurysm/dissection or you have been detected to have one, you could consult your physician or the Aneurysm Clinic.
A detailed physical examination and blood investigation should be done for assessing the fitness of the patient for treatment.
If there is no contraindication a computed tomography angiography (64 slice minimum) should be performed.
A CT scan will give the location, exact dimensions and relationship of the aneurysm to the main branch arteries of the body. This will help plan whether treatment is required and what sort of treatment should be planned.
In few cases if a CT scan cannot be performed or if additional information is required, then a digital subtraction angiogram (DSA) or a magnetic resonance imaging (MRI) may be done.
Size is an important criterion for aneurysms. The normal aorta in the chest measures 2.5-3.2 cms, and in the abdominal aorta measures 1.8-2.3 cms. If the thoracic or abdominal aneurysm is less than 4.5 cms in its maximum diameter, then medical management is advised with regular radiologic follow up. If the size is greater than 4.5cms then treatment should be planned.
In cases of dissections, detailed discussion and planning has to be done to decide the treatment, which are now successfully treated by the endovascular method.
The traditional treatment for aortic aneurysms has been surgery, where via an incision in the chest or the abdomen, the aneurysmal segment is bypassed using a vascular graft (tube made of cloth). However surgery can be associated with risks and complications; such as prolonged general anaesthesia, blood loss, infection.
Hence a minimally invasive procedure such as endovascular stent grafting can also be performed to treat these aneurysms with excellent results; which are equivalent to surgery.
Here through a small hole in the groin arteries a specialized device, known as an aortic stent graft in introduced into the artery, and this prevents flow of blood into the aneurysm.
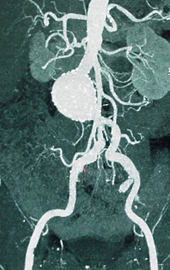
65 Year old doctor, incidental detection of a large infrarenal abdominal aortic aneurysm on a routine health check up

Successful exclusion of the aneurysm with an endovascular stent graft
An aortic stent graft is a device made up of stents covered by a surgical vascular graft; this can be introduced through the artery and placed across the aneurysmal segment. The stents act as anchors and the vascular graft directs the blood away from the aneurysm.

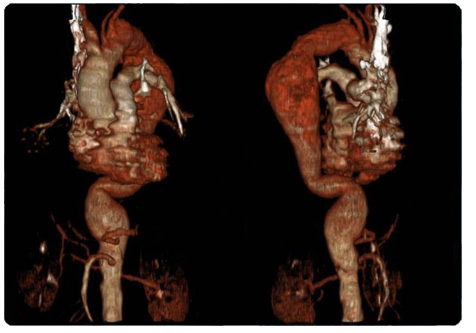
73 year man, presented with back pain, on imaging detected to have a large descending thoracic aortic aneurysm, extending distal to the left subclavian artery, upto the celiac artery.

Treatment with multiple thoracic stent grafts.
Depending on the location of the aneurysm in relation to the branch arteries, combination treatment known as hybrid procedures can be performed. Here a less risky surgery is done and in the same sitting an endovascular graft is inserted. This is to preserve blood in the main branch arteries to the vital organs of the body and also treat the aneurysm.
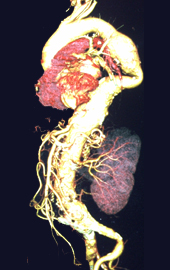
63 year old lady, detected to have a large 6.5cms thoraco-abdominal aortic aneurysm, extending, distal to the leftsubclavian artery to the aortic bifurcation, on pre-operative work up for a knee surgery.

Two year follow up CT angiogram, after a hybrid endovascular repair. Surgical bypasses to the celiac, SMA, left renal, with endovascular exclusion of the aneurysm.
If surgery is contraindicated then for abdominal aorta aneurysm where the aneurysm involves the intestine and renal arteries, a highly specialized procedure known as fenestrated/branched stent grafting can also be performed. Fenestrated devices have holes in the graftsynchronized to the visceral ostia to allow the inclusion of the renal and intestinal vessels. THE FIRST ONE IN THE COUNTRY WAS PERFORMED BY THE ANEURYSM CLINIC.

38 year man, end stage renal disease, detected to have a juxtarenal abdominal aortic aneurysm, involving both common iliac arteries.

Successful exclusion of the aneurysm with a fenestrated graft to the celiac and superior mesenteric arteries and an iliac branched graft to the right common iliac artery.
Aortic dissections can also be treated by the endovascular method, where the tear in the aorta is closed by the stent graft, thereby increasing flow in the narrowed distal artery and the arteries supplying the intestine, liver, kidneys and legs.
Traumatic tears to the aorta, which are life threatening and occur mainly with high impact collisions can be successfully treated by aortic stent grafts.
The aneurysm clinic is a super-speciality clinic which addresses, the comprehensive treatment for aortic aneurysms and dissections.
The clinic comprises of a team of Interventional Radiologists, Cardiovascular Surgeons, Vascular Surgeons and Intensivists, who have been trained in aneurysm care. Surgical and endovascular care is offered by the clinic, with a stress of life style management and follow up (post treatment).
The doctors associated with the clinic have the maximum experience in endovascular and surgical treatment of aortic aneurysms; with the first successful fenestrated and branched aortic graft performed in the country. In lieu of their vast experience, cases have also been performed in South Asia (Singapore, Thailand, Indonesia, Malyasia).
Till August 2014 performed a total of 546 endovascular procedures for aortic aneurysms.